


Where Have You Been?
I have grappled with how much and what specifically to share here. Do I focus on the pathogenesis of MS, how treatments work, and why certain treatments aren’t available to everyone? Prior to being diagnosed, I couldn’t tell you anything about MS. Conversely, should this just be the way to chronicle the steps that I am taking, the challenges I face, or even what symptoms are like on a day-to-day basis? Being vulnerable here has difficult for a many reasons, but I am over it. I know who my subscribers are: If we were sitting down face-to-face, I would share more than this with every one of you. As I wrote the first few posts, it felt like I was writing about someone else. I shouldn’t be that detached from my own story.
I also struggle with the expectations I place on myself. For better or worse, I care about my writing. I care about what others think and I want them to enjoy reading or glean something from it. If there are skills I want to improve, I will seek out authorities to observe. As I desire to write at a high level, I intentionally read higher-quality authors and journalists for the same reason. While these writers stylistically influence and push me, I need to realize that I am not them. Each piece that I publish cannot, and will not, be perfect. I don’t have an editor and self-editing is a tedious process with inevitable mistakes. I’ve come to the realization that I don’t need an editor. This particular medium is less formal, I’m just leaning into and embracing it. I am not writing for a publication, I don’t have the resources those writers have. While I dream of writing at a high level, I’ve learned to accept that I will make mistakes. Those mistakes will not be the end of the world, nor will people think less of me over of a grammatical or spelling error. Writing here is an intimidating but an already rewarding adventure. Granted, coming to the realization that any mistake made on the initial post will live in a subscriber’s inbox forever is sobering. Can I make a change on this site? Absolutely. I cannot go into your inbox and change an error that I published in that first version.
Coming Out
My initial appointment with my new neurologist was on March 2, 2020. I had two topics that I wanted to cover with them. We needed to decide which drug would I go onto next and I needed to tell them that I would be seeking HSCT. For some odd reason ($$$), neurologists aren’t particularly supportive of HSCT as a treatment for MS. Why would you ask? First, the neurologist must agree that MS should be treated by both a neurologist and hematologist. Multiple sclerosis is an autoimmune disorder where certain white blood cells are incorrectly attacking and damaging the central nervous system. This is not just about nerves and declining neurological function. Furthermore if the transplant is successful, patients do not require the care of a neurologist. Only a primary care physician and hematologist/oncologist (if needed), monitors or provides care to the patient post-transplant. It makes sense. The practice loses a customer, err patient. Why would any person with a financial interest in a neurology practice be in favor of this?
I left the appointment with two main concerns. First, my fear over potential opposition to HSCT was real. It was in their medical opinion that undergoing a stem cell transplant was far too risky nor did it have the clinical track record that DMTs (drugs) have. While I preferred Rituxan (rituximab) for my next DMT, they strongly advocated for a drug called Tysabri (natalizumab). On the subject of the transplant, I was assured that the safer alternative was to “be on a medication that has been tested and widely used.” Also, if I was hoping for a new cutting edge treatment I should be looking into a study like this, not a stem cell transplant. By the way, that study is a phase-two trial testing the remyelination of nerves in rats. In. Freaking. Rats. This is maybe ten years away from human phase-three trials; let alone being approved by the FDA, added to insurer’s standards of care, and made broadly available to the public. Leaving the appointment, I told them that I would still be seeking the transplant and I did not want to start Tysabri, I wanted to go onto Rituxan instead.
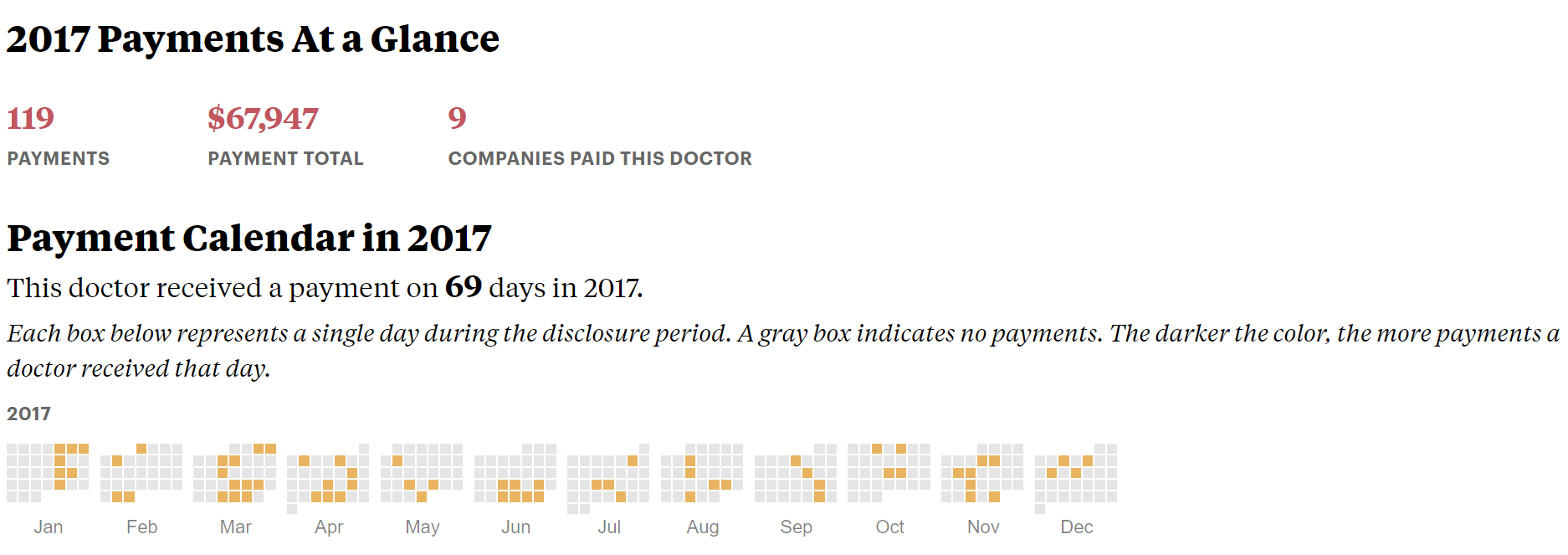
The consistent pushing of a particular drug made me skeptical. I think we have all heard stories about doctors being paid by pharmaceutical and medical device companies. After a quick Google search, I learned pharmaceutical companies are compelled by law (thankfully) to disclose the physician, date, amount, service provided, and which specific drug or device it was in regards to. Annually they compile all of these payments and file financial disclosure forms, which are public record. These public records are aggregated by ProPublica’s tool called Dollars for Docs, which makes them searchable and accessible to the average person. A search revealed that in 2017 and 2018, a total of nine pharmaceutical companies paid my neurologist $100,173 for their promotional speaking and consulting fees, along with any travel expenses. Simple arithmetic revealed that thirty-five percent ($34,758) of those dollars were paid to them by Biogen, the manufacturer of Tysabri. Interestingly, the drug that I wanted to start taking is manufactured by Genentech, who paid my doctor a total of twenty dollars in 2017 and another twenty-one dollars in 2018. Forty-one dollars versus thirty-five thousand. How could any logical person not question everything they say? Thankfully they obliged, and I had my first infusion of Rituxan a few days later.
Lazy Summer
While the pandemic summer was boring, it was a relaxing. I was lucky enough to keep working, spend time with my girls, and fish with my Dad. After spending June and July investigating treatment options in the US, I found the Colorado Blood Cancer Institute (CBCI) and released my records for their evaluation. Unbeknownst to me, I had not met a single point of the inclusion criteria: I had only failed one drug. While my records were in review at CBCI, I (thankfully?) had another relapse. I now experienced proximal weakness in my left arm and numbness on my face. Like most other relapses, these new symptoms accompanied the disabling symphony of my other neurological symptoms. I started a course of high-dose steroids after being diagnosed with a relapse. My neurologist questioned if the Rituxan was still in my system, so they ordered a blood test that checks B lymphocyte levels (what Rituxan destroys). If the blood test showed B cells in my bloodstream, this wouldn’t be a DMT failure. This indicates that the B cells repopulated earlier than expected and I would need another dose of Rituxan sooner than expected. After the ten day wait, we got the results from the Mayo Clinic, the B cells had not repopulated. I had a relapse while my drug was doing what it was supposed to be doing. I failed my second drug. Failure and a relapse has never felt so good.

Following the relapse and the review of my medical records, I was accepted as a potential candidate for transplant. The next step was to obtain the referral to CBCI, which worried me. I needed to convince my neurologist that they should refer me to an out-of-state clinic for a treatment that they don’t support. Attempting to give myself every advantage possible, I made an appointment for an in-office visit. I believe it is more difficult to deny someone asking for help in person than over the phone or webcam. During the appointment, I informed them of my acceptance by CBCI as a potential candidate for a transplant. I needed a referral to the clinic, and I was hopeful that they would refer me. Not only did they agree, there wasn’t even a protest. Responding they said, “I am not going to hold you back from a treatment you believe is right for you. I am just forewarning you, I have never heard of an insurance company paying for stem cells even though we know they work.” ARE. YOU. KIDDING. ME. Even though we know they work?!? Less than six months ago, you asked me why I would try an “experimental treatment” like HSCT and now we know they work? Oh, and on the subject of insurance companies not paying for stem cells? Challenge accepted.
Referred and Denied v1.0
My neurologist faxed in the paperwork, and CBCI submitted the referral with an office visit authorization request. During this appointment, Dr. Nash would review my medical records and describe the procedure. If still a candidate, he would order the pre-transplant testing and the actual transplant. Unfortunately, none of this happened. The insurance company denied the referral for just the office visit. In the denial they said CBCI was out of network, but that Cancer Care Northwest (CCNW) (where I live) was in my network. Too bad that CCNW is strictly an oncology practice. They are not qualified nor do they have the capability to treat MS patients. This had to be a mistake. I quickly filed the appeal believing once an actual human read everything, the error would be realized and I would move on. Man alive, was I naïve. Seventy-two hours later, the appeal was denied. This time, they stated I had not exhausted all of the available pharmaceutical interventions. According to their “criteria,” I was not a candidate for a transplant. I was advised to ask my neurologist for a letter stating I had failed a second high-efficacy drug and should be evaluated for a transplant. Along with the letter, I would need a new referral which had not been denied yet. My doctor agreed to write the letter and faxed over a second referral to CBCI. (Early Sept. 2020)
With this new documentation, CBCI requested the authorization for office visits again. Now, the insurance company wouldn’t even let them submit the new referral and letter. CBCI was informed that I would need a “Visiting Member Number,” or member ID for Colorado, for the referral to be processed. I obtained the Colorado member ID and sent it to CBCI, it only took a few afternoons sitting on hold. Two days later, I received an email informing me that the insurance company would not accept the referral from an out-of-state provider. After a few more hours on hold, it was explained that if I would like a referral processed, it needed to be from a neurologist in Colorado. After contacting CBCI and asking if there were any friendly neurologists in my network, I had a name.

I celebrated Pearl Harbor Day by establishing care with my new Colorado PCP. Beginning the appointment, I explained the situation and the need for a referral to a Colorado neurologist. The Colorado PCP was wonderful. They went through my health history and agreed to write the referral. Before we ended, they asked if there was a particular neurologist that I wanted to see. I provided the neurologist’s name and information. On New Years Eve, I had a telehealth visit with the Colorado neurologist. They took a detailed health history, reviewed imaging, and other test results; we even discussed my hopes and expectations for treatment. At the end of the visit my CO neurologist said, “I think it is perfectly reasonable for you to be evaluated for a transplant. You clearly have an aggressive course of MS, you have failed two drugs and your disability level has progressed. I am excited for you. I hope that this is something that can happen. You do realize that if this (the transplant) works it’s a cure, right?” A physician, no a neurologist, use the (good) C word with me. I was shocked. I don’t think my two neurologists could be any more different. Why can’t my new neurologist in Colorado be my doctor all the time?
Two weeks into the new year, I called the insurance company to confirm the receipt of the new referral. I was told it was under review and they have another eight business days to approve or deny the referral, unless I had an appointment regarding the referral. I was then informed of the greatest loop-hole ever: if I had a scheduled appointment inside of those eight days, I could call twenty-four hours before and they expedite the review of the referral. After a quick phone call, I had an appointment booked two days later. I called to expedite the referral the next morning and by 3pm I was approved for fifteen office visits. Holy. Shit. It was finally happening. Whitney and I were actually meeting with Dr. Nash and his team the next afternoon. We were both excited until going over the transplant process. This wouldn’t take the thirty to thirty-five days like it does in Russia or Mexico. Here, the whole process takes roughly ninety days. Coming to the realization that I wouldn’t be with Whitney and Sloan for three months was terrifying. The sheer volume of moving parts was daunting. The first twenty to twenty-five days and the last thirty to thirty-five days of the transplant are outpatient where I must provide my own housing, special diet, and a caregiver who is available/with me twenty-four hours per day. At the end of an overwhelming hour-and-a-half, Dr. Nash ordered the pre-transplant labs and transplant.
Referred and Denied v2.0
If I was able to sit down with each of you individually, I could tell you so much more than I can publicly write here. Just over two weeks ago (2/18/2021) I officially received the denial letter. One of the challenges MS-ers experience is the difficulty in making plans. Somehow, they always change. Whether fairly simple like a family gathering or bigger and more complex decisions, like family planning. My chosen defense mechanism has been to just expect that everything that can go wrong, will go wrong. Yes, taking that Murphy of an attitude is dark, but has saved me from a ton of disappointment and heartbreak. Family, friends, and even the clinic were somewhat confident that we had hit our last hurdle and that it would be approved. I wouldn’t let myself think it was going to get approved; I truthfully expected a denial. This process is emotionally challenging enough, let alone if I actually let myself believe it would be approved. I have hit every possible roadblock on this journey so far, why would it be different now? Even with my defense mechanisms and lowered expectations through the process, it is still mentally and emotionally exhausting. Strangely, I was relieved after receiving the denial letter for two reasons. I had this overwhelming feeling of finally. I could start to move forward and play the cards that I have been holding for the last six months. After settling down enough to read the letter, I went from being relieved to excited.


Reading through the letter, you see the transplant is listed as being “Not Medically Necessary Member Liable.” Amazing. I have a Neurologist in Washington State, another Neurologist in Colorado (both of which you required me to see), and my transplant Oncologist/Hematologist who all believe that this procedure is medically necessary. Later in the letter, the explanation for denial is different than the initial reason. Instead of being not medically necessary, the reason changed to “multiple sclerosis is not a covered indication for a stem cell transplants” and the requested provider is out of network.
Let’s get this straight. If MS is not a covered indication for a stem cell transplant, why did the neurologist that you required I see to get the referral say I should be evaluated for a transplant? Also, why would you (insurance company) approve the fifteen office visits for me to be evaluated if my illness isn’t a covered indication based on the clinical criteria? This was the best denial letter that I could have received when it comes to the appeal process. Game on.

Silver Lining
Like I said above, hitting every roadblock is emotionally exhausting to not just me, but my wife and family as well. We have prayed through this arduous process that we would learn about the system to help others get this, or other, life-changing treatments. My greatest fear as a parent is that my daughter (and hopefully another child one day) would be diagnosed with MS. IF, God forbid, they are diagnosed in the future, I want them to have access to this treatment without the shit I have dealt with. I want my friends with MS to have access to this treatment. Everyone with MS should have access to the most effective treatments available, period.
A couple of hours after I electronically received the denial letter, CBCI received theirs as well. In addition to the denial letter, Dr. Nash received an email from an Executive-level MD at the nationwide parent of my insurance company. This executive invited Dr. Nash to speak at their national semi-annual conference on previous clinical trial data, the upcoming BEAT-MS trial, and his personal experience treating autoimmune patients. My insurance company wasn’t just seeking information, they are considering adding HSCT to their national standards of care for MS patients. This physician and my insurance company were only contacting Dr. Nash because they just had a patient (me) try to get a stem cell transplant from his clinic and it was denied.
Prior to this, I was in my emotional basement. I don’t think it is ridiculous or abnormal for someone going through challenges like this to feel down or depressed. There are somewhere between sixty-thousand and one-hundred thousand MS patients in the United States who are insured by my insurance company. The potential of putting a crack or hole in this wall was just the motivation I needed. I am beyond stubborn. I’m described as hard-headed, a bull in a China shop, and unafraid to speak my mind. If I can use these normally abrasive characteristics for good, I’m all in. We are putting together the appeal documents, the letter, and will be submitting it to my insurance company in the next week or so.
Housekeeping
I am currently writing a deep-dive into the business of treating MS. I am often asked if this is such an efficacious treatment, why isn’t it widely available? Is it an issue of regulatory burdens and the FDA? Has it not been approved by the FDA? Amazingly enough, no. That would have been a relatively benign answer. In my opinion, the reasons behind HSCT not being widely available to the population are far darker and sinister than that of regulatory failure. I have been working on this project for a while and I am excited to share it with you. Instead trying to weave the whole thing, or portions into other posts, I am just going to write a post (or posts) just on that topic. I don’t know when I will finish it, but I am mentioning it as a form of accountability.
While this is long, my goal was to finish bringing you all up to date with my MS story. March is Multiple Sclerosis Awareness (and Education) Month. The next three posts this month will focus on how the immune system damages those of us with MS and some of the symptoms that I experience on a daily basis.
Thank you for going on this ride with me. I appreciate each and every one of you.
- Aaron

So glad to hear your stubbornness is paying off! Get ‘em tiger!
I think I've learned more about Multiple Sclerosis reading your posts than dealing with my own diagnosis and treatment. Fighting for the right to HSCT treatment could mean everything to people dealing with this disease in the future. You and your girls seem to be one heck of a team and I wish you all the success and good health you all deserve. If there's anything I can ever do to help, please ask so I can also be a part of the fight!